
More Information
Submitted: November 02, 2022 | Approved: November 14, 2022 | Published: November 15, 2022
How to cite this article: Marian MR, Gabriel K, Andrei MM, Eniko P, Mircea T, et al. Dynamic knee valgus in anterior cruciate ligament non-contact injury and reinjury in professional female athletes. Determinant or not? J Nov Physiother Rehabil. 2022; 6: 029-033.
DOI: 10.29328/journal.jnpr.1001048
Copyright License: © 2022 Marian MR, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Dynamic knee valgus; ACL reconstruction; Female athletes

Dynamic knee valgus in anterior cruciate ligament non-contact injury and reinjury in professional female athletes. Determinant or not?
Melinte Razvan Marian1-4*, Koszorus Gabriel2, Melinte Marian Andrei5, Papp Eniko3, Tabacar Mircea1 and Zolog-Shiopea Dan1,4
1Puls-Regina Maria Hospital, Targu Mures, Romania
2Fizionova Rehabilitation, Targu Mures, Romania
3Dimitrie Cantemir University, Targu Mures, Romania
4Humanitas Hospital, Cluj Napoca, Romania
5University of Medicine and Paharmacy Targu Mures, Romania
*Address for Correspondence: Melinte Razvan Marian, Puls-Regina Maria Hospital, Targu Mures, Romania, Email: mmelinte@yahoo.de; razvanmel@xnet.ro
Dynamic Knee Valgus (DKV) is correlated with both, Anterior Cruciate Ligament (ACL) injury and hip and ankle disorders in female athletes and has a more significant prevalence compared with male athletes because of numerous factors.
The aim of this study is to determine if the connexion between DKV, landing errors, and non-contact ACL injury and re-injury in high-performance, adult, female team sport athletes can be eliminated by changing the frontal plane movement pattern and the landing errors during the rehabilitation process (RHB), a process which was focussed on dynamic knee stability with multidimensional single-leg jump landing training, on 3D knee balance improvement and multistimulus perturbation challenges and tasks,+ eccentric & concentric exercise, strength & conditioning, aerobic training that lasted from 26 - 44 weeks.
Assessing and eliminating-reducing DKV during the RHB is mandatory in lowering the re-rupture rates in female professional athletes after ACL surgery and in preventing opposite knee trauma.
Dynamic Knee Valgus (DKV) is a complex anatomic and biomechanic pathology that is associated with both, Anterior Cruciate Ligament (ACL) injury and hip and ankle disorders [1], weaker hip abductor muscles-gluteus medius and magnus, larger pelvis with increased Q angle and flat forefoot are all conditions which can determine this biomechanical abnormality-and this condition is much more prevalent in female athletes and has a bigger functional impact in female athletes compared with male athletes because of additional biomechanical and hormal factors like -lower levels of testosterone, hormonal inhibitions and variations during luteal phases of menstrual cycles, hormonal induced ligament laxity for females who come back in the first 12 - 16 months after childbirth- and habitual factors- wrong biomechanical jump and landing patterns developed at early ages Figure 1.
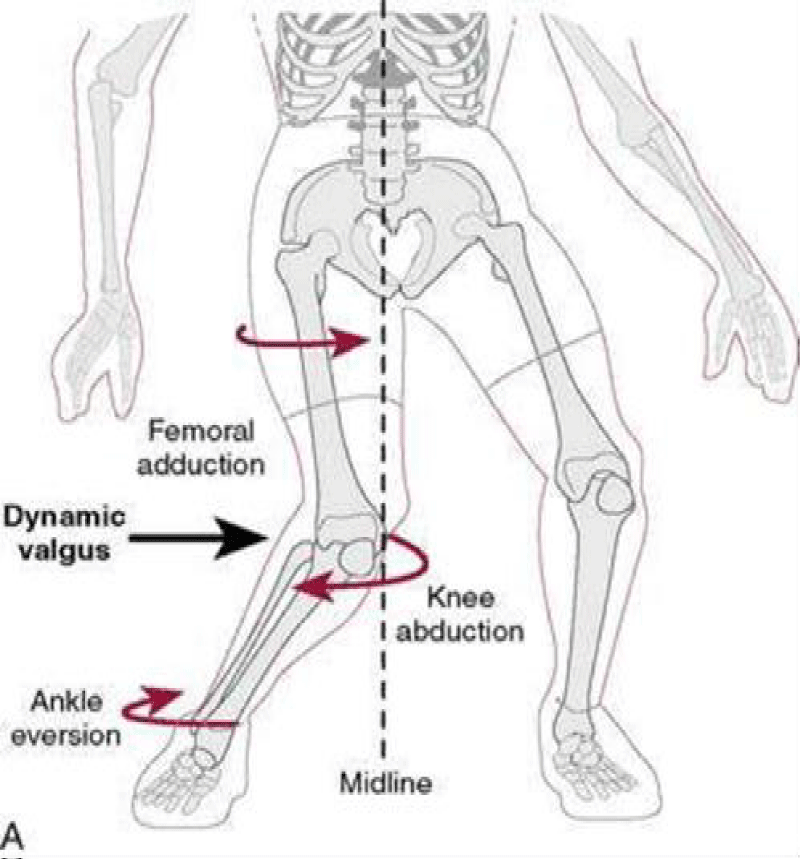
Figure 1: [5].
The aim of this study is to determine if the connexion between DKV, landing errors, and non-contact ACL injury and re-injury in high-performance, adult, female team sport athletes can be eliminated by changing the frontal plane movement pattern and the landing errors during the rehabilitation process by both plyometric training and hip stability development [2].
This is aimed at reducing very high rates of reinjury after ACL reconstruction in females, especially in young adults.
We examined and included in our study 41 female professional athletes, between 18 and 34 years old, practicing team sports in the first national leagues of handball (n = 27), basketball (n = 11), soccer (n = 2) and 1 volleyball (n = 1), all operated or re-operated because of non-contact ACL injury between 2019-2022. Our follow-up was a minimum of 36 months in all cases.
Primary ACL surgery was done by the same surgeon and an arthroscopic technique was performed, we used a Soft Tissue graft, the revision was performed with a patella bone graft; resorbable interference screws were used in all cases for tibial fixation, and femural fixation was realized with TightRope Button - Arthrex. No graft under 8 mm diameter was used, all grafts between 7 mm – 8 mm were reinforced using Fibertape -Arthrex, also grafts under 7 mm were braided to obtain 8 mm grafts Figures 2,3.
Figure 2: Graft Augmentation.
Figure 3: Graft Braidings.
All athletes were investigated during the RHB, between 12 - 18 weeks-WKS-after surgery for isometric strength [measured on EasyTorque 3.0 from Tonus producer -E.T.3.0]-and for altered frontal plane knee movements and abnormal leg biomechanics with the Landing Error Scoring System(LESS), bilateral -indicating increased level of DKV-which was present in 34 cases (83%) Table 1-scores higher then 6-high AClL Injury risk & DKV.
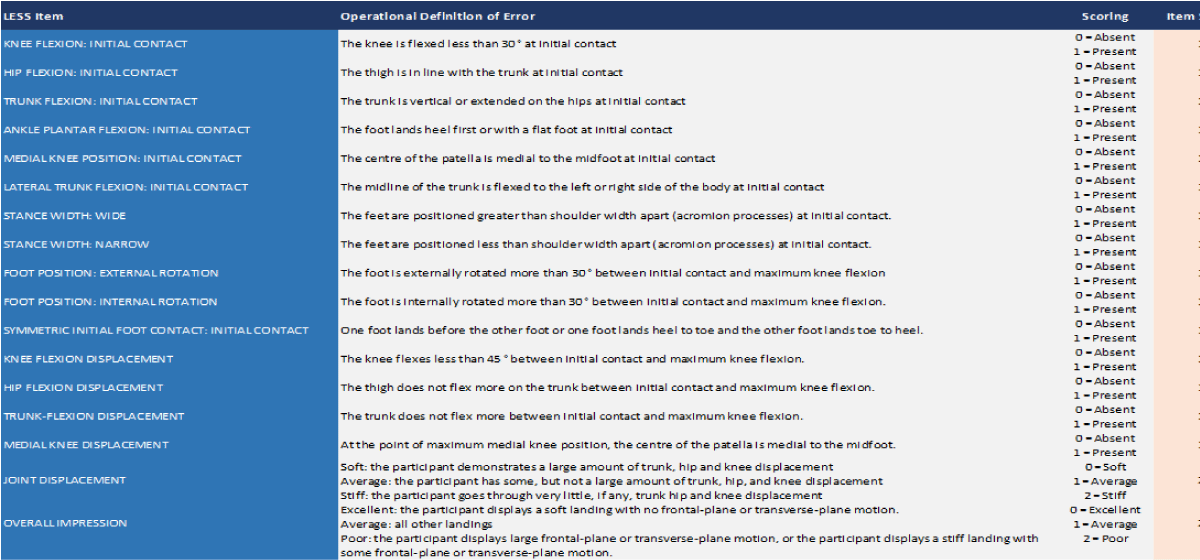
Table 1: LESS scoring [3].
Flat Forefoot was ruled out in 33 of these cases-97%, the remaining case was orthotic corrected and was included in the study Figures 4,5.
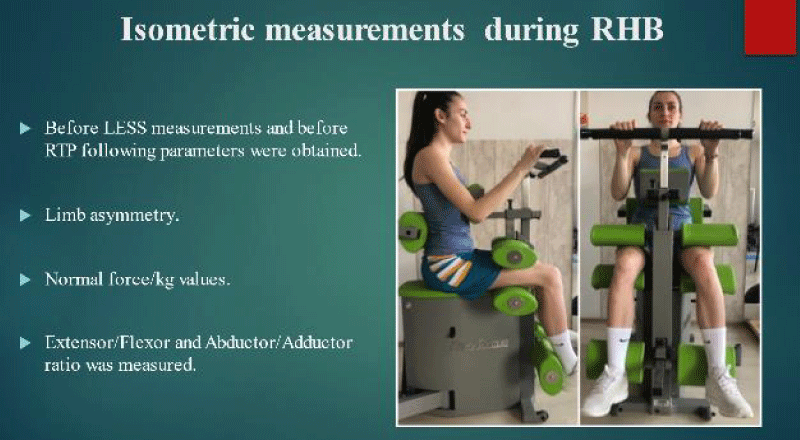
Figure 4: Isometric measurements.
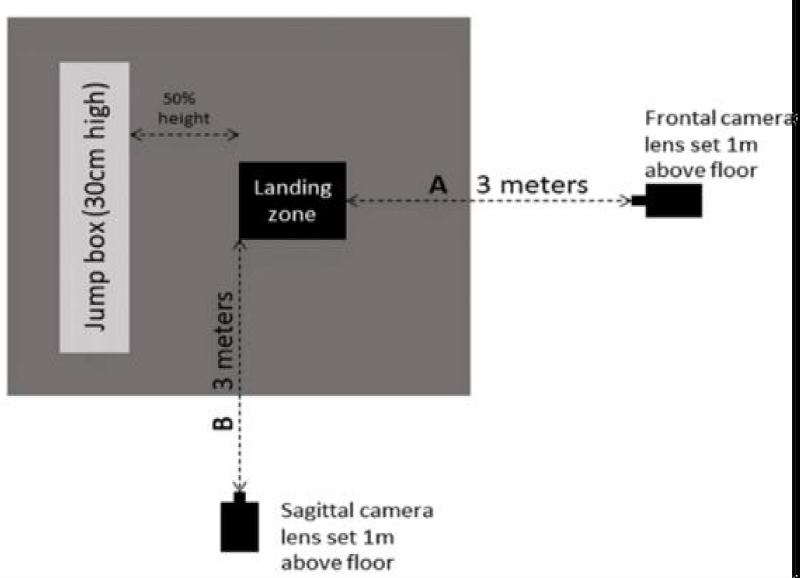
Figure 5: LESS measurements.
First presented in 2009, the Landing Error Scoring System (LESS)* is a clinical tool used to assess jump-landing biomechanics. It was developed to identify individuals at risk of anterior cruciate ligament (ACL) injury and is performed with a subject completing a Drop-Vertical Jump (DVJ) whilst video recorded from two planes (frontal and sagittal).
Being an easier, faster, and cheaper field-based variant of a complete biomechanical assessment, it can be performed without expensive laboratory equipment [3].
Measurement of the knee valgus angle is one of the main factors which can be objectively used in correction evolution [4].
The RHB process was focused on dynamic knee stability with multidimensional single-leg jump landing training from varying heights-0,3 - 0,9 m, on 3D knee balance improvement-BOSU ball, Balance Boards, and multistimulus perturbation challenges [5] and tasks [throwing, catching balls, Therabands, pulling in different directions, pushing, pulling by trainer],+eccentric & concentric exercise, strenght & conditioning, aerobic training and lasted from 26-44WKS with normalized LESS score[lower than 5].
Multivariate analysis of Landing Kinetic factors during the rehabilitation process showed significant differences between two LESS scores at different time frames so an altered landing mechanism is considered a predictor of non-contact knee injuries such as ACL rupture [6] this is why it is so important to be addressed Figure 6.
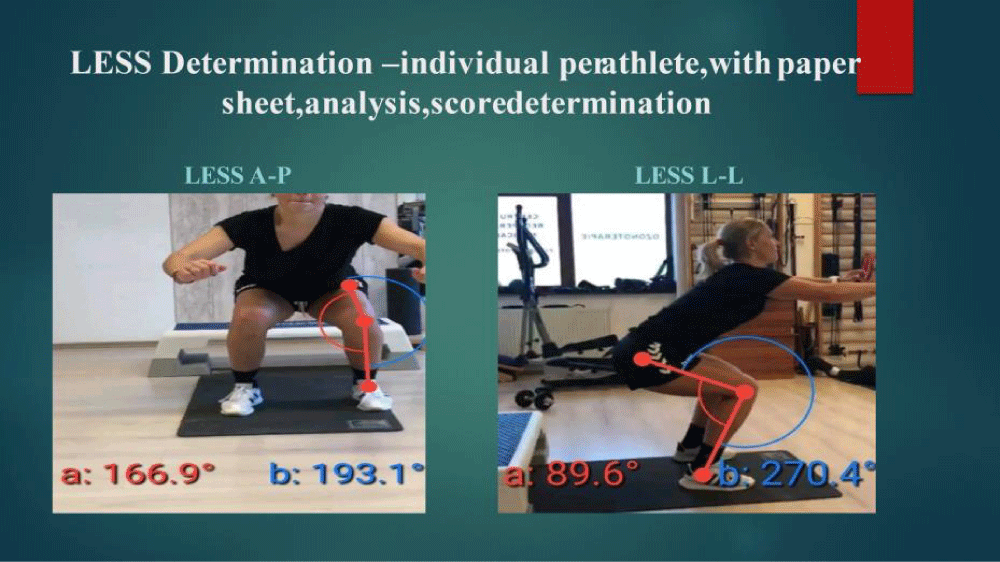
Figure 6: LESS Determination-individual parathlete, with paper sheet, analysis, score determination.
Average Return To Play was in 32.1 weeks (WKS) with an SD of +1,2 WKS ranging from 28-35 WKS, after tests on “ EasyTorque” 3. o-Tonus- passing criteria were more than 95% bilateral limb symmetry.
The ”Triple One-Leg Hop Test”-“Cross-over One-Leg Hop Test” at 95% - 98% on both legs-normal cardiovascular endurance-Cooper test was used for assessment and psych-ological readiness to perform again was reached in all cases. Reaching the preinjury level of individual performance took between 40-48WKS and was considered when the player was integrated into normal team rotation, which preinjury number of game minutes&eficiency, points depending on the sport.
From 34 cases, 1 athlete re-injured after RHB, friendly game, at 32WKS after surgery (3%), 2 athletes injured after RHB, in competition -the opposite ACL in the first 48WKS after ACL surgery (6%)-1 basketball player did not return to professional level mostly because of psychological factors-fear of reinjury, lack of motivation-1 handball player quit the sport after re-injuring in competition at 50WKS, deciding to have a child.
Diagram 1 shows us in the first group of columns the total number of ACL injuries with red and with blue the number of patients who had DKV when injured.
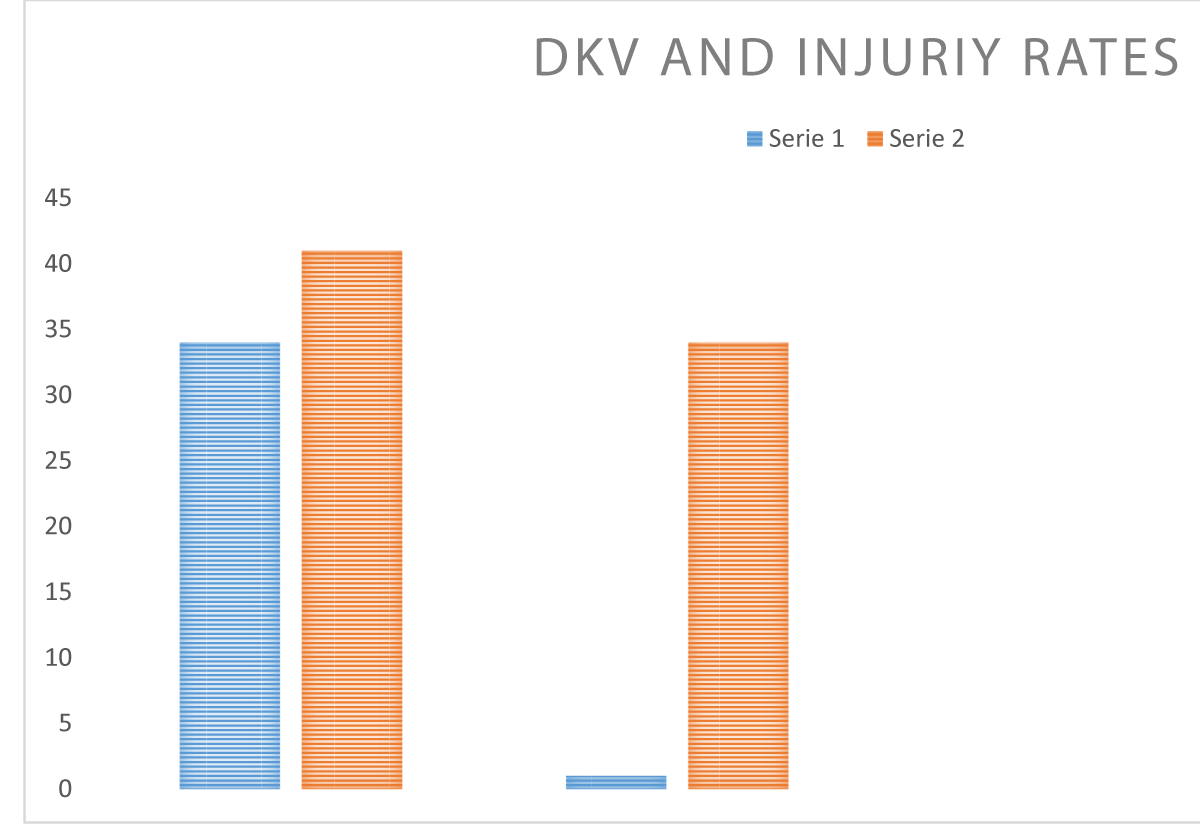
Diagram 1: Total ACL Injuries-red /DKV athletes-blue; Reinjury rates in patients which corrected DKV-blue.
The second row of columns shows with red the number of patients with an ACL injury who successfully returned to high-performance sports and with blue the re-injured ones after our program.
Considering the fact that female athletes with dynamic knee valgus are considered a high-injury risk category for ACL ruptures, especially during team-pivoting-contact sport, we consider that trying to correct through Neuroplasticity and specific rehabilitation (Neuroplasticity - which is the capacity of the brain to learn new movement patterns and to establish new connexions in the motor cortex through synaptogenesis and neurogenesis) and trying to positively alter the biomechanics throughout the rehabilitation process is an achievable goal.
In Table 2 we have the LESS score measurement of our female athletes and the type of sport they are performing in, in the interval of 12 - 18 weeks after surgery, the higher the score the more dynamic knee valgus and landing errors exist.
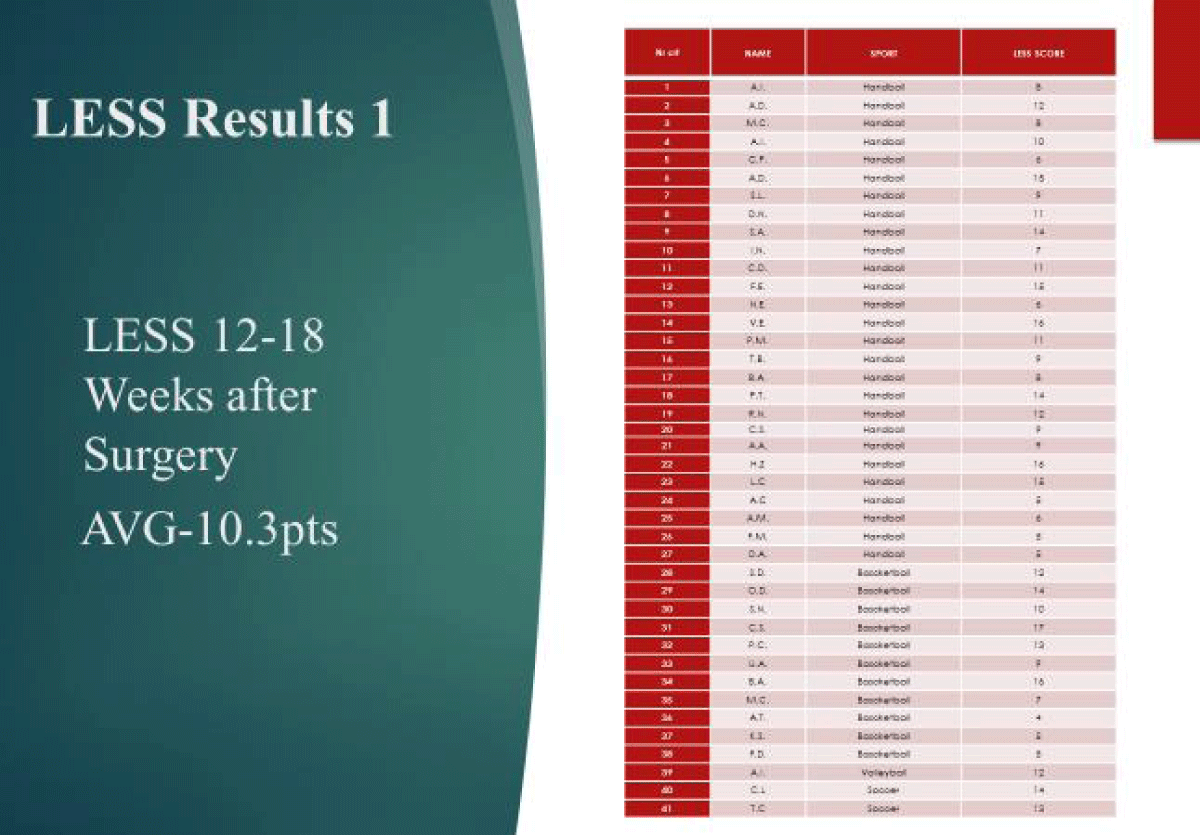
Table 2: LESS Results 1 LESS 12-18 Weeks after Surgery AVG-10.3 pts.
In Table 3, we observe that the LESS score has improved through specific plyometric, neuropeptide, and strength training which means that landing errors diminished drastically, and we have better biomechanics, more pelvic stability, and hip abductor strength.
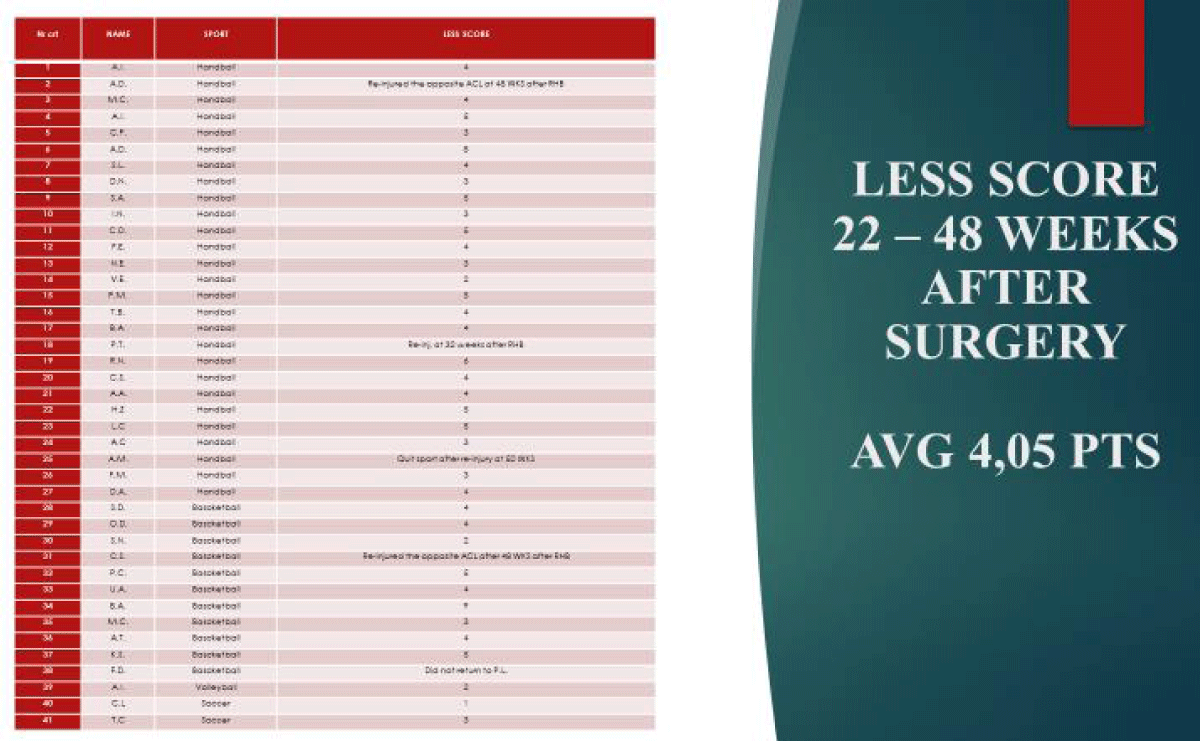
Table 3: LESS Score 22 -48 weeks after surgery AVG 4,05 PTS.
The re-injury complication rates on operated leg- 2/34 = 5,8% and on the opposite side 2/34 = 5,8% are lower than published data [7] varying from 7% - 15% ipsilateral and 8% - 10% contralateral in the first year. This is statistically significant and could be related both to the longer RHB period and DKV correction, a process that is individualized and complex [8]. Anyway, still highest rate of reinjury after ACL surgery is observed in young, female athletes who participate in pivoting contact sports [9]. Energy absorbing strategies during landings, single or bilateral leg landings must be also learned in order to reduce stress o the knee - especially axial loading and forces which would increase valgus angle [10].
Rates of primary ACL injuries in female sports and especially in female contact team sports are still very high despite advances in surgical techniques, materials, and in the rehabilitation process-sports like women’s handball, soccer, and basketball being particularly affected [5].
Assessing and eliminating-reducing DKV during the RHB process is mandatory in lowering & re-rupture rates in female professional athletes after ACL surgery and in preventing opposite knee trauma.
Also, we strongly believe that return to sport criteria which include assessing DKV and hop tests, an additional MRI for assessing graft vascularization, and integration should be used in allowing athletes to return to the competition level.
All must be done to prevent an injury and re-injury – a well-designed program like FIFA 11 is very effective and should be implemented [11].
- Tamura A, Akasaka K, Otsudo T, Shiozawa J, Toda Y, Yamada K. Dynamic knee valgus alignment influences impact attenuation in the lower extremity during the deceleration phase of a single-leg landing. PLoS One. 2017 Jun 20;12(6):e0179810. doi: 10.1371/journal.pone.0179810. PMID: 28632776; PMCID: PMC5478135.
- Wilczyński B, Zorena K, Ślęzak D. Dynamic Knee Valgus in Single-Leg Movement Tasks. Potentially Modifiable Factors and Exercise Training Options. A Literature Review. Int J Environ Res Public Health. 2020 Nov 6;17(21):8208. doi: 10.3390/ijerph17218208. PMID: 33172101; PMCID: PMC7664395.
- Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE Jr, Beutler AI. The Landing Error Scoring System (LESS) Is a valid and reliable clinical assessment tool of jump-landing biomechanics: The JUMP-ACL study. Am J Sports Med. 2009 Oct;37(10):1996-2002. doi: 10.1177/0363546509343200. Epub 2009 Sep 2. PMID: 19726623.
- Asaeda M, Nakamae A, Hirata K, Kono Y, Uenishi H, Adachi N. Factors associated with dynamic knee valgus angle during single-leg forward landing in patients after anterior cruciate ligament reconstruction. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2020 Aug 24;22:56-61. doi: 10.1016/j.asmart.2020.07.002. PMID: 32913714; PMCID: PMC7451847.
- Dynamic knee valgus in anterior cruciate ligament non-contact injury and reinjury in professional female athletes. Determinant or not? Melinte RM, Zolog D, Koszorus G, Sandru D (Targu Mures, Romania)- Football medicine meets the universe of sport. XXVIII Isokinetic Medical Group Conference. 27-28-29 April 2019. Wembley Stadium, London (Anglais) Brochéde G. S. Roi (Sous la direction de), S. Della Villa (Sous la direction de)ISBN-10: 8860285909ISBN-13: 978-8860285904
- Reyhaneh M, Fariba B, Reza R , Hooman M, Katarzyna K. Investigating the landing kinetics factors and preparatory knee muscle activation in female handball players with and without dynamic knee valgus while performing single-leg landing. Biomedical Human Kinetics. 2021; 13. 155-162. 10.2478/bhk-2021-0019.
- Weiss K, Whatman C. Biomechanics Associated with Patellofemoral Pain and ACL Injuries in Sports. Sports Med. 2015 Sep;45(9):1325-1337. doi: 10.1007/s40279-015-0353-4. PMID: 26130304.
- Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of Secondary Injury in Younger Athletes After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis. Am J Sports Med. 2016 Jul;44(7):1861-76. doi: 10.1177/0363546515621554. Epub 2016 Jan 15. PMID: 26772611; PMCID: PMC5501245.
- Webster KE, Feller JA. Exploring the High Reinjury Rate in Younger Patients Undergoing Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2016 Nov;44(11):2827-2832. doi: 10.1177/0363546516651845. Epub 2016 Jul 7. PMID: 27390346.
- Dadfar M, Soltani M, Novinzad MB, Raahemifar K. Lower extremity energy absorption strategies at different phases during single and double-leg landings with knee valgus in pubertal female athletes. Sci Rep. 2021 Sep 1;11(1):17516. doi: 10.1038/s41598-021-96919-y. PMID: 34471189; PMCID: PMC8410826.
- Sadigursky D, Braid JA, De Lira DNL, Machado BAB, Carneiro RJF, Colavolpe PO. The FIFA 11+ injury prevention program for soccer players: a systematic review. BMC Sports Sci Med Rehabil. 2017 Nov 28;9:18. doi: 10.1186/s13102-017-0083-z. PMID: 29209504; PMCID: PMC5704377.